Fit2Sit PATIENT ADMITTANCE PROCESS FOR
CURRENTLY ENROLLED HOSPITALS
ETOBICOKE GENERAL HOSPITAL
1 – Paramedics and patient enter through the ambulance entrance and continue to the main (public) waiting room
2 – Assist patient to the end of the “greeting line” and inform them that once “greeted” they will be instructed on where to sit
3 – Provide brief verbal report and Fit2Sit Paramedic Report to the next available triage nurse
4 – Crew marked Transfer of Care (HTOC)
5 – Leave health card and personal belongings with the patient
6 – Update PTOC status
HUMBER RIVER HOSPITAL
1 – Paramedics and patient enter through the ambulance entrance and continue to the main (public) waiting room
2 – Assist patient with completing the electronic screening kiosk process, for chief complaint select other and input EMS + chief complaint (i.e. EMS – headache)
3 – Assist patient to chairs or wheelchair in the main ED waiting room
4 – Provide brief verbal report and Fit2Sit Paramedic Report to the next available triage nurse
5 – Crew marked Transfer of Care (HTOC)
6 – Leave health card and personal belongings with patient
7 – Update PTOC status with Clearing Coordinator
MICHAEL GARRON HOSPITAL
1 – Paramedics and patient enter through the general ED entrance and check in at the pre-registration window
2 – Assist patient to chairs or wheelchair in the main ED waiting room
3 – Provide brief verbal report and Fit2Sit Paramedic Report to the next available triage nurse
4 – Crew marked Transfer of Care (HTOC)
5 – Leave health card and personal belongings with patient
6- Update PTOC status with Clearing Coordinator
MOUNT SINAI HOSPITAL
1 – Paramedics and patient enter through the main ED entrance and assist patient with “ED Check-in”. Paramedics will advise check-in that patient is Fit2Sit.
2 – Assist patient to chairs or wheelchair in the main ED waiting room
3 – Provide brief verbal report and Fit2Sit Paramedic Report to the next available triage nurse.
4 – Crew marked Transfer of Care (HTOC)
5 – Leave health card, personal belongings, and queue ticket number with patient
6 – Update PTOC status with Clearing Coordinator
NORTH YORK GENERAL HOSPITAL
1 – Paramedics and patient enter through the main ED (public) entrance and report to the swipe nurse
2 – Provide brief verbal report and Fit2Sit Paramedic Report to the swipe nurse
3 – Crew marked Transfer of Care (HTOC)
4 – Assist patient to chairs or wheelchair in the main ED waiting room
5 – Leave health card and personal belongings with patient
6 – Update PTOC status with Clearing Coordinator
SAINT JOSEPH’S HOSPITAL
1 – Paramedics and patient enter through ambulance entrance and continue to the main (public) waiting room
2 – Obtain a triage number from the ticket machine and assist patient to chairs or wheelchair in the main ED waiting room
3 – Provide brief verbal report, triage number and Fit2Sit Paramedic Report to the next available triage nurse
4 – Crew marked Transfer of Care (HTOC)
5 – Leave health card, triage number ticket and personal belongings with patient
6 – Update PTOC status with Clearing Coordinator
SAINT MICHAEL’S HOSPITAL
1 – Paramedics and patient enter through the main ED entrance
2 – Assist patient to chairs or wheelchair in the general seating area of the main ED waiting room
3 – Identify registration desk to the patient and “when required by registration” direct patient to self-register – the patient will be instructed by hospital staff where to sit following registration
4 – Provide brief verbal report and Fit2Sit Paramedic Report to the next available triage nurse
5 – Crew marked Transfer of Care (HTOC)
6 – Leave health card and personal belongings with patient
7 – Update PTOC status with Clearing Coordinator
SCARBOROUGH BIRCHMOUNT HOSPITAL
1 – Paramedics and patient enter through the main ED (public) entrance
2 – Assist patient to the RED chairs or wheelchair behind the screener
in the main ED waiting area
3 – Provide brief verbal report and Fit2Sit Paramedic Report to the triage nurse
4 – Crew marked Transfer of Care (HTOC)
5 – Leave health card and personal belongings with patient
6 – Update PTOC status with Clearing Coordinator
SCARBOROUGH CENTENARY HOSPITAL
1 – Paramedic and patient enter through the main ED entrance
2 – Assist patient to chairs or wheelchair in the main ED waiting room
3 – Provide brief verbal report and Fit2Sit Paramedic Report to the next available triage nurse
4 – Crew marked Transfer of Care (HTOC)
5 – Leave health card and personal belongings with patient
6 – Update PTOC status with Clearing Coordinator
SCARBOROUGH GENERAL HOSPITAL
1 – Paramedics and patient enter through the ambulance entrance and continue to the main (public) waiting room
2 – Assist patient to the RED chairs or wheelchair in the main ED waiting area
3 – Provide patient with triage number from RED dispenser located in ED (public) waiting area
4 – Provide brief verbal report and Fit2Sit Paramedic Report to the next available triage nurse
5 – Crew marked Transfer of Care (HTOC)
6 – Leave health card and personal belongings with patient
7 – Update PTOC status with Clearing Coordinator
SUNNYBROOK HOSPITAL
1 – Paramedics and patient enter through the main ED (public) entrance
2 – Assist patient with completing the electronic screening kiosk process and to the chairs or wheelchair in the main ED waiting room
3 – Provide brief verbal report and Fit2Sit Paramedic Report to the next available triage nurse
4 – Crew marked Transfer of Care (HTOC)
5 – Leave health card and personal belongings with patient
6 – Update PTOC status with Clearing Coordinator
TORONTO GENERAL HOSPITAL
1 – Paramedics and patient enter through the ambulance entrance and assist the patient through the screening process with the volunteer located by the public entrance
2 – Assist patient to chairs or wheelchair in the main ED waiting area
3 – Provide brief verbal report and Fit2Sit Paramedic Report to the next available triage nurse
4 – Crew marked Transfer of Care (HTOC)
5 – Leave health card and personal belongings with patient
6 – Update PTOC status with Clearing Coordinator
TORONTO WESTERN HOSPITAL
1 – Paramedics and patient enter through the main ED (public) entrance
2 – Assist patient to chairs or wheelchair in the “Triage Seating” section (section 1) in the main ED waiting room
3 – Provide brief verbal report and Fit2Sit Paramedic Report to the next available triage nurse
4 – Crew marked Transfer of Care (HTOC)
5 – Leave health card and personal belongings with patient
6 – Update PTOC status with Clearing Coordinator
REFERENCE MATERIAL
This document includes additional information regarding updates to the Fit2Sit program, and supports the related memorandum titled Fit2Sit Update released on February 24, 2023.
Note: Updated to include additional questions indicated in red
Q1. What are the benefits of Fit2Sit?
A1. Fit2Sit helps to reduce the amount of time Paramedics spend in hospital and improve the flow of patients in the ED. This benefits TPS by increasing opportunities for meal breaks, going home on time, station time and downtime, and improved ambulance availability in the community. It provides hospitals the benefit of lower transfer of care (TOC) times, which positively impacts ED performance.
Q2. Does Fit2Sit meet all Ministry of Health (MOH) requirements?
A2. Yes. The Fit2Sit program does not eliminate any of the requirements set out in the BLS Patient Care Standards. The Memorandum of Agreement between TPS and participating hospitals allows the triage report to be split into three components rather than one long verbal report.
Q3. Has Fit2Sit proven to be safe?
A3. Between December 6, 2022 and January 16, 2023:
* 566 patients were enrolled in Fit2Sit with documented tracking numbers.
* Only 3.1% of total audited calls required further clarification and or investigation.
* One patient was flagged at triage as being outside of the program criteria. The call was reviewed and found the patient had met criteria at time of TOC. The patient was appropriately triaged and treated based on the new presentation.
Q4. Is the Paramedic expected to wait in the queue in order to provide the verbal report and Fit2Sit card to the triage nurse?
A4. No. The Paramedic is expected to present themselves to the next available triage nurse. They are not to interrupt a nurse if they are actively triaging a patient and they are to be professional and courteous at all times. The verbal report and completed card are designed to cause minimal intrusion to the triage nurse and flow of patients in the emergency department.
Q5. What if the triage nurse does not want to accept the patient?
A5. Fit2Sit does not require the triage nurse to accept the patient. In the agreed upon process the Paramedic is only required to identify the patient as Fit2Sit and provide the verbal report and Fit2Sit card to the triage nurse. If there is disagreement between the Paramedic and the triage nurse that cannot be resolved, please contact your Superintendent or the Deputy Commander for assistance.
Q6. Who is responsible for the patient once they are offloaded to the waiting room?
A6. Fit2Sit empowers Paramedics to make the decision to offload appropriate patients to the ED waiting rooms, where hospital staff are expected to be responsible for the patient, as they would be for any other walk-in patient.
Q7. What if the patient complains about being left in the waiting room?
A7. Paramedics should inform the patient of the Fit2Sit process prior to the arrival at the hospital. This may need to be reiterated once triage has been completed to ensure the patient understands the process. Adhering to the Fit2Sit criteria will help safeguard Paramedics from complaints regarding the patient’s final location in the ED. Paramedics are encouraged to contact a Superintendent if they have any concerns following a call.
Q8. When does TOC start for Fit2Sit patient?
A8. Hospital Transfer of Care (HTOC) occurs immediately after the Paramedic provides the verbal report and hands the Fit2Sit card to the triage nurse. Paramedic TOC (PTOC) should be declared immediately following this process.
Q9. Does the patient have to remain on the stretcher
A9. No. The BLS standards state that the paramedic shall “for all CTAS 3-5 patients transport the patient to and from the ambulance using the appropriate lift, carry or ambulatory assistance with respect to the situation, the patient’s clinical condition, or for patient comfort”1 This means that, if appropriate for the situation, a patient may remain ambulatory throughout the transport.
Q10. Do Paramedics need to take a Blood Glucose on every Fit2Sit patient?
A10. No. Paramedics are to follow the same standard of practice as with any other patient they treat. Blood sugars are taken if hypoglycemia is suspected or is being ruling out. A blood sugar is not required for Fit2Sit patients unless there is clinical evidence to support taking one.
Q11. How do Paramedics fill out the Fit2Sit section on the ePCR?
A11. Paramedics are to fill out the Fit2Sit section on the ePCR as follows:
- Does not meet Fit2sit criteria
* Select this if patient is excluded due to CTAS or inclusion/exclusion criteria - Patient enrolled in Fit2Sit
* Select if the patient is left in the main waiting room to self-triage and short verbal report + Fit2Sit Paramedic Report was left with the triage nurse
****Enter tracking number**** - Not enrolled but meets Fit2Sit criteria
* Patient meets the Fit2Sit Criteria however you triage the patient as per our normal practice
** Document brief explanation and why patient not enrolled
Q12. If patient meets Fit2Sit criteria and is not enrolled, why does a reason have to be entered in the ePCR?
A12. There may be times where a patient meets the Fit2Sit criteria however they are not suitable to be left to self-triage. Paramedics are asked to provide an explanation on why it was not appropriate for the patient to self-triage. This provides valuable insight for program evaluation and may lead to changes if common trends are identified.
Q13. What if the triage nurse does not agree with patient offload to the waiting room?
A13. The three most common errors noted in Fit2Sit documentation are:
- Patient being marked as “Enrolled in Fit2Sit” and without a tracking number entered.
- Patient being marked as “Enrolled in Fit2Sit” when the Paramedic triaged the patient as per our normal practice.
* These patients are to be documented with a final disposition of a room or bed and not the waiting room. - Patients fall outside of the age criteria and are unaccompanied.
* If a patient is outside of the age criteria but accompanied by another party, please be sure to document this in the ePCR.
Q14. Where can Paramedics obtain more Fit2Sit Cards?
A14. If there are no Fit2Sit cards in the ambulance, please contact a District or Hospital Task Force Superintendent for replacement cards.
DOWNLOAD PDF:
UHN Stabilization Centre Operational Medical Directive
University Health Network Stabilization Centre Medical Directive
A Paramedic may transport a patient to the University Health Network Stabilization Centre
under the auspices of this Medical Directive if certified and authorized.
INDICATIONS
Toronto Paramedic Services may transport a patient to the Stabilization Centre established by the University Health Network (UHN) at 750 Dundas Street West (Toronto) for patients who are suspected to be under the influence of alcohol (ethanol) or an opioid, in whom there are no contraindication, immediate threat to life, or need for time-sensitive medical or surgical intervention.
Paramedics may bypass to the UHN Stabilization Centre in lieu of transporting the patient to a hospital’s emergency department if the patient meets the clinical conditions in this medical directive.
CONDITIONS
Paramedics may bypass a hospital emergency department and transport the patient directly to the UHN Stabilization Centre if the patient meets the following inclusion criteria:
-
- adult (age ≥16 years) with known or suspected alcohol (ethanol) or opioid intoxication
CONTRAINDICATIONS
Transport to the Stabilization Centre is contraindicated if a patient has any one of the following:
- History or evidence of significant recent trauma or injury
- Respiratory distress
- Requires acute intervention by paramedics or hospital staff for life-threatening or time
sensitive condition - Administration of symptom-relief medication* by bystanders, first responders or
paramedics - New focal neurological deficit
- Known or suspected toxic ingestion or exposure not related to alcohol (ethanol) or opioid
- Exposure to pepper spray or other crowd-control agent
- Exhibits ongoing agitation or violent behaviour
- Requires physical and / or chemical restraint
- CTAS 1
- Abnormal vital sign (see below)
*Patients who require or received any one of the following medications are NOT ELIGIBLE for transport to the Stabilization Centre:
- salbutamol
- epinephrine
- nitroglycerine
- glucagon
- oral or parenteral dextrose
- ketorolac (toradolTM)
- diphenhydramine (benadrylTM)
- dimenhydrinate (gravolTM)
Note: patients who require or received acetaminophen or ibuprofen tablets by mouth or naloxone by any route ARE ELIGIBLE for transport to the Stabilization Centre.
In order to be appropriate for the Stabilization Centre, the patient must be able to ambulate and verbalize UNLESS the patient’s inability to do so is related to ethanol or opioid ingestion. If the inability to ambulate or verbalize is due to any other cause, the patient is
NOT ELIGIBLE for transport to the Stabilization Centre.
If a patient exhibits agitation or violent behaviour, paramedics may use their discretion and request a police escort to ensure patient and paramedic safety. If a police escort is required, the patient is NOT ELIGIBLE for transport to the Stabilization Centre.
Vital sign parameters
The patient is excluded from being transported to the Stabilization Centre if he / she exhibited any one of the following vital signs at any point while in paramedic care:
- Pulse <50 or >110 beats per minute
- Respirations <10 or >24 breaths per minute
- Systolic blood pressure <100 or >150 mm Hg
- Oxygen saturation <93% on room air or requirement for supplemental oxygen to maintain >93%
- Temperature <35.5 or >38oC
- Point of care glucose <5.0 or >14.0 mmol/l
TREATMENT and PRECAUTIONS
The paramedic will obtain a complete medical history, including intoxicant use, perform patient assessment, and obtain vital signs (pulse, respirations, blood pressure, oxygen saturation, temperature, GCS) and point-of-care glucometry. The assessment and findings must be documented in the electronic patient care record.
Signs and symptoms of intoxication may include slurred speech, disinhibited behaviour, central nervous system depression, and altered coordination. In order to be appropriate for the Stabilization Centre, the patient’s primary source of intoxication must be ingested ethanol or opioid.
- Ingested ethanol intoxicants such as hairspray, mouthwash, and hand sanitizer are also appropriate for transport to the Stabilization Centre.
- Ingested methanol (windshield washer fluid) or ethylene glycol (antifreeze) are NOT appropriate for transport to the Stabilization Centre.
- Inhaled intoxicants such as solvent, gasoline, paint and lacquer thinner are NOT appropriate for transport to the Stabilization Centre.
While the inability to ambulate or verbalize may be due to intoxication, these may also mimic a head injury or stroke. If a head injury or stroke is suspected, transport to the Stabilization Centre is NOT appropriate.
If the patient has been exposed to capsaicin (pepper spray, bear spray, mace, or similar) or other crowd control agent, decontamination is required. Transport to the Stabilization Centre is NOT appropriate.
A patient who originally presents with agitation or violent behaviour may be suitable for transport following de-escalation through paramedic interventions. If paramedics require a police escort following de-escalation, transport to the Stabilization Centre is NOT appropriate.
Manifestation of serious head injury may be identical to, or clouded by, substance intoxication. Paramedics should be reminded that mixed and / or unknown overdoses can cause multiple signs and symptoms, and that some medical conditions (e.g. hypoglycemia, electrolyte deficiency, hypovolemia, arrhythmia, seizure, sepsis, meningitis) may result in symptoms similar to intoxication. If the assessment suggests an acute injury or medical condition, paramedics should consider management via established medical directives for these purposes (e.g. seizures, hypovolemia, arrhythmias) and transport the patient to a hospital.
If the patient’s condition changes at any point in time during transport, the paramedic must reassess eligibility for transport to the Stabilization Centre. If no longer eligible, the paramedic must inform the destination coordinator, advise of the change in condition, and request a hospital destination.
On arrival at the Stabilization Centre, paramedics will transfer patient care to the Stabilization Centre intake staff. Paramedics must obtain a final and complete set of vital signs (pulse, respirations, blood pressure, oxygen saturation, and GCS) just prior to transfer of care, document these on the electronic patient care report, and note the time of transfer of care.
APPROVAL
Dr. Russell MacDonald, MD MPH FCFP FRCPC DRCPSC
Medical Director, Toronto Paramedic Services
Version 20221118
Approved 2022 November 18
DOWNLOAD PDF:
UHN Stabilization Centre Operational Medical Directive
University Health Network
Stabilization Centre Medical Directive Quick Reference
Paramedics may bypass a hospital emergency department and transport the patient directly to the UHN SC if the patient meets the following criteria:
Conditions
* Patient age 16 or greater
* Known or suspected alcohol (ethanol) intoxication
Vital Signs (at all times)
* Pulse 50-110 beats per minute
* Respirations 10-24 breaths per minute
* Systolic Blood Pressure * 100-150 mm Hg
* Oxygen Saturation 93% or greater on room air
* Temperature 35.5C – 38C
* Point of care glucose 6-14 mmol/l
Contraindications
X Any vital sign outside of the ranges above, at any time in paramedic care
X CTAS 1
X Respiratory distress
X Trauma/injury – evidence or history of recent & significant
X Life-threatening or time-sensitive condition requiring acute intervention
X New inability to verbalize/ambulate, unrelated to alcohol
X New focal neurological deficit
X Known or suspected toxic ingestion or exposure not related to alcohol (ethanol)
X Known or suspected opioid use
X Naloxone administration from any source
X Pepper spray or crowd-control agent exposure
X Ongoing agitated/violent behaviour
X Requires restraint
X Pt received any of: salbutamol, epinephrine, nitroglycerine, glucagon, dextrose,
ketorolac, diphenhydramine, dimenhydrinate
In order to be appropriate for the Stabilization Centre, the primary reason for the patient’s inability to ambulate or verbalize must be ingested ethanol.
If the inability is due to any other cause, the patient is NOT ELIGIBLE for transport to the Stabilization Centre.
V.2022-12-05
CLICK HERE FOR THE MEDICAL DIRECTIVE
DOWNLOAD PDF:
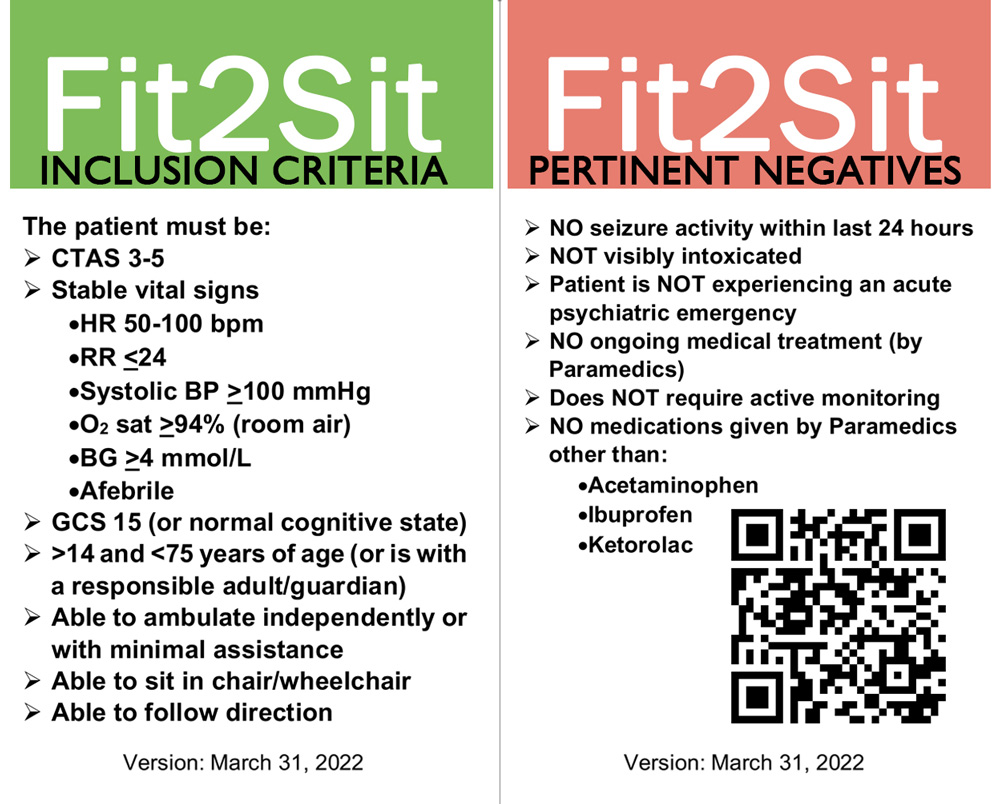
Fit2Sit_Quick_Ref_Card.pdf